Idaho Child Lead Risk Assessment and Blood Lead Testing Recommendations
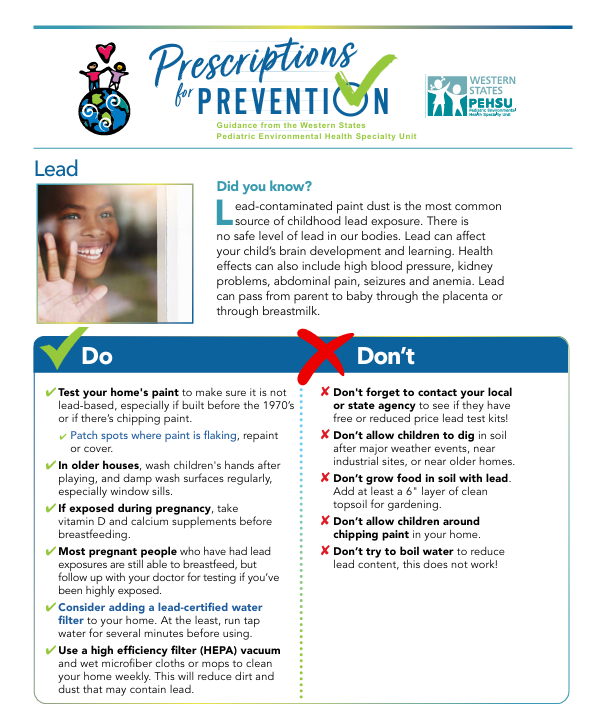
Children exposed to lead are vulnerable to long-term health and developmental effects, including intellectual and behavioral deficits. Conducting l…
Region 10
| Lead